

Introduction
As artificial intelligence reshapes diagnostic medicine, healthcare systems worldwide are discovering a powerful truth: deep learning algorithms can outperform conventional lab testing. Indeed, they deliver greater clinical precision. Moreover, they enable earlier disease detection. And crucially, they generate measurable cost savings.
Real-World Breakthroughs
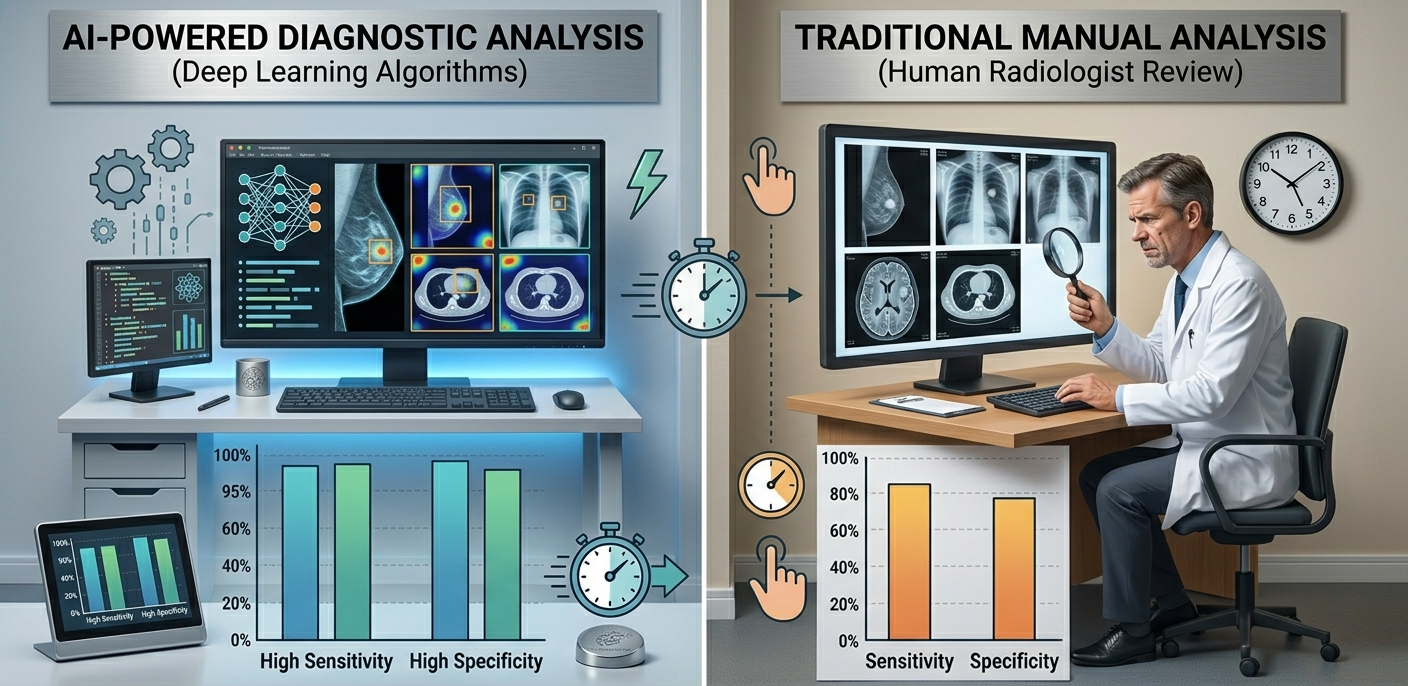
For example, AI-driven imaging now spots subtle cancers human eyes might miss. Similarly, algorithmic electrocardiograms predict heart failure months in advance. Consequently, the old model of reactive testing is fading. Thus, AI flips reactive medicine into preventive action. Indeed, early detection becomes the new standard—not the exception revolutionizing healthcare.
Current Implications and Challenges
So what does this mean today? Quite simply: better outcomes, lower costs, and faster decisions. Patients gain time. Providers gain accuracy. Policymakers gain leverage. Yet challenges remain — data privacy, algorithm bias, and regulatory lag. Nevertheless, the trajectory is clear. Deep learning is not a futuristic promise. It is a present reality — with profound implications for patients, providers, and policymakers today.

The Diagnostic Crossroads
Every year, global healthcare systems process billions of laboratory tests. Moreover, the cost burden associated with this diagnostic infrastructure is staggering — the U.S. alone spends over $100 billion annually on clinical laboratory services. Meanwhile, deep learning, a sophisticated subset of artificial intelligence, is rapidly demonstrating that machines can read medical images, analyze biomarkers, and flag disease risks with an accuracy that matches or even surpasses experienced clinicians.
The Shift from Traditional Labs to AI Diagnostics
Consequently, a critical financial and clinical debate has emerged at the heart of modern medicine: Should healthcare providers continue investing heavily in traditional laboratory infrastructure, or should they pivot aggressively toward AI-driven diagnostics? This question, furthermore, is not merely theoretical. It directly impacts hospital budgets, insurance reimbursements, patient wait times, and — most importantly — survival rates.
Therefore, this analysis examines the financial impact of deep learning diagnostics in contrast to traditional lab tests, focusing specifically on medical precision, early detection capabilities, and advances in diagnostic imaging. In addition, we explore the regulatory frameworks that now govern AI medical devices and consider what the transition means in practical terms for healthcare institutions worldwide.
“The greatest opportunity to reduce suffering and cost in medicine lies not in new drugs, but in better, faster, and earlier diagnosis.”
Eric Topol, M.D.— Author, Deep Medicine; Director, Scripps Research Translational Institute
“Artificial intelligence is not going to replace doctors. But doctors who use artificial intelligence will replace doctors who don’t.”
Bertalan Meskó, M.D., Ph.D.— Medical Futurist; Director, The Medical Futurist Institute
Nevertheless, it is equally important to acknowledge that precision alone does not determine financial viability. Implementation costs, training requirements, data infrastructure, and regulatory compliance all factor into a complete economic analysis. Therefore, examining the hidden costs embedded in the traditional diagnostic chain is essential before drawing conclusions.
The Hidden Costs of Traditional Laboratory Testing
At first glance, traditional laboratory testing appears to be a mature, cost-controlled system. However, a deeper financial audit reveals multiple layers of hidden expenditure that significantly inflate the true cost-per-diagnosis. These include reagent waste, equipment calibration, quality assurance protocols, inter-laboratory sample transportation, and workforce overheads associated with skilled technicians.
The Catastrophic Cost of False Negatives
Moreover, false negatives in traditional testing carry catastrophic downstream costs. When a standard complete blood count or imaging review misses an early-stage malignancy, the patient typically presents months or years later with advanced disease. At that stage, treatment protocols are not only more aggressive but also substantially more expensive. Accordingly, a single missed pancreatic cancer diagnosis, for example, can result in treatment costs exceeding 300,000,compared tounder12,000 for early-stage surgical resection.
The Speed Penalty of Physical Handling
Additionally, traditional testing depends on physical sample handling — a process that introduces both time delays and contamination risks. Turnaround times for complex diagnostic panels frequently range from 24 to 72 hours. Meanwhile, point-of-care AI systems integrated with imaging devices can generate preliminary risk assessments within seconds of data acquisition. This speed difference has direct financial implications in emergency medicine, where faster diagnosis reduces intensive care unit (ICU) admission rates and shortens hospital stays.
“We are drowning in information, while starving for wisdom. The world henceforth will be run by synthesizers — people able to put together the right information at the right time.”
E.O. Wilson— Biologist & Two-time Pulitzer Prize Laureate
Direct Labor Cost Reduction
Furthermore, staffing costs constitute one of the largest components of traditional diagnostic spending. In the United States, a licensed clinical laboratory scientist earns a median annual salary of approximately
75,000, and high-volume reference laboratories employ hundreds of such professionals. In contrast, a fully deployed AI diagnostic module, once trained and validated, can process tens of thousands of tests daily with minimal variable cost per analysis, typically reducing per-test costs by 50–80% within three to five years of deployment.
Upfront Investment and Long-Term TCO
However, it would be misleading to suggest that deep learning eliminates all overhead. On the contrary, initial deployment of AI diagnostic systems requires significant upfront investment in computing infrastructure, data labeling, model validation, and cybersecurity. Therefore, a thorough total cost of ownership (TCO) analysis over a 10-year horizon consistently demonstrates that AI-augmented diagnostics become cost-superior beyond the third year of deployment in high-volume healthcare environments.
Deep Learning in Diagnostic Imaging: Redefining Radiology Economics
Diagnostic imaging represents the single largest and most financially significant domain for AI disruption in medicine. Globally, radiology departments process over 3.6 billion imaging studies annually. Consequently, even marginal improvements in reading efficiency translate into billions of dollars in system-wide savings. Deep learning algorithms — particularly convolutional neural networks (CNNs) and vision transformers — now demonstrate the ability to triage urgent findings, auto-detect anomalies, and generate structured radiology reports with minimal human oversight.
AI Advances in Medical Imaging
AI systems trained on large imaging datasets excel across multiple modalities. For lung cancer screening via chest CT, deep learning models (e.g., LUNA16-trained networks) achieved an AUC of 0.944, surpassing the radiologist panel’s 0.883. FDA-cleared AI now autonomously diagnoses diabetic retinopathy from fundus photos, expanding access in primary care.
AI triage also reduces missed critical findings caused by fatigue or high caseloads. Research in Radiology found that AI-assisted triage cut time-to-intervention for pulmonary embolism by 11 minutes, improving survival and saving ICU costs.
“Medicine is a science of uncertainty and an art of probability. Artificial intelligence gives us the power to tip that probability dramatically in the patient’s favor.”
William Osler, M.D.— Father of Modern Medicine (adapted in the context of AI diagnostics)
Furthermore, workflow automation enabled by AI dramatically reduces the administrative burden of radiology departments. Automated report generation, anomaly flagging, and PACS (Picture Archiving and Communication System) integration allow radiologists to focus on complex, high-value interpretations rather than routine screenings. As a result, radiologist productivity increases by an estimated 30–40%, effectively expanding departmental capacity without proportional increases in headcount or physical infrastructure.
Regulatory Frameworks, Ethical Standards, and Real-World Deployment
The financial viability of deep learning in diagnostics depends on regulatory and ethical compliance. In the U.S., the FDA has cleared over 950 AI/ML medical devices, mostly for imaging. The EU’s AI Act classifies diagnostic AI as high-risk, requiring clinical validation, risk management, and post-market surveillance—costs that established developers can manage. The WHO emphasizes equity, transparency, and accountability in AI diagnostics. Though non-binding, this guidance influences national health system procurement. Developers that adopt explainable AI (XAI)—providing interpretable clinical justifications—gain regulatory favor and institutional trust, accelerating adoption and lowering deployment costs.
“For every complex problem, there is an answer that is clear, simple, and wrong. Good regulation of AI in medicine must be sophisticated, adaptive, and evidence-driven.”
H.L. Mencken— American journalist and cultural critic (principle adapted to AI regulation context)
Nevertheless, regulatory timelines represent one of the most significant barriers to rapid AI diagnostic deployment. The average FDA 510(k) clearance pathway for a moderate-risk AI diagnostic device currently requires approximately 12–18 months and costs between $500,000 and $2 million in regulatory preparation. However, once cleared, the commercial scale-up economics are highly favorable, since the same validated algorithm can be deployed across thousands of institutions with minimal incremental cost. This dynamic fundamentally differentiates AI diagnostics from traditional reagent-based laboratory systems, where each incremental test carries variable consumable costs.
Additionally, real-world deployment experience is now generating robust economic evidence. The Mayo Clinic, Cleveland Clinic, and Massachusetts General Hospital have all published data demonstrating that AI-assisted diagnostic workflows reduced downstream testing redundancy by 18–27% and significantly decreased unnecessary specialist referrals. Furthermore, in resource-limited healthcare systems across sub-Saharan Africa and Southeast Asia, cloud-based AI diagnostic tools are providing specialist-level diagnostic capabilities at a fraction of the cost of maintaining local laboratory infrastructure, redefining healthcare access economics globally.
Conclusion: Toward a Financially Smarter, Clinically Sharper Healthcare System
The financial case for deep learning in medical diagnostics is not merely speculative — it is rapidly becoming empirically irrefutable. Across precision oncology, diagnostic imaging, pathology, and preventive screening, AI systems consistently demonstrate the ability to reduce per-diagnosis costs, accelerate clinical decision-making, and improve patient outcomes through earlier, more accurate disease detection.
However, the transition from traditional laboratory infrastructure to AI-augmented diagnostics is neither instantaneous nor without financial risk. Institutions must navigate upfront capital investment, workforce retraining, regulatory compliance, cybersecurity obligations, and the cultural shift required to integrate algorithmic recommendations into clinical practice. Therefore, a phased implementation strategy — beginning with high-volume, high-cost diagnostic categories such as radiology triage, pathology slide analysis, and diabetic screening — offers the most favorable risk-adjusted return on investment.
Moreover, policymakers, hospital executives, and technology developers must work collaboratively to ensure that AI diagnostic adoption proceeds equitably. Because diagnostic inequality already disproportionately burdens under-resourced populations, the deployment of accessible, affordable AI tools must be designed as a mechanism for expanding diagnostic coverage — not concentrating it further among wealthy healthcare systems.
Ultimately, the question is not whether deep learning will transform medical diagnostics. It already is. The more pressing question — for healthcare leaders, investors, engineers, and clinicians alike — is how quickly and how wisely this transformation will be managed. Because the financial stakes, patient lives, and the future architecture of global healthcare all depend on the answers we choose today.
“The function of science is not merely to describe the world, but to heal it. Every algorithm that correctly identifies a cancer one day earlier is a life better lived.”
Francis Collins, M.D., Ph.D.— Former Director, National Institutes of Health (NIH)
References
- RAJPURKAR, P.; CHEN, E.; BANERJEE, O.; TOPOL, E. J. AI in health and medicine. Nature Medicine, vol. 28, 2022, pp. 31–38. doi: 10.1038/s41591-021-01614-0.Link
- ESTEVA, A. et al. Dermatologist-level classification of skin cancer with deep neural networks. Nature, vol. 542, 2017, pp. 115–118. doi: 10.1038/nature21056.Link
- McKINSEY GLOBAL INSTITUTE. Transforming Healthcare with AI: The Impact on the Workforce and Organizations. New York: McKinsey & Company, 2020. Available at: https://www.mckinsey.com/industries/healthcareLink
- OBERMEYER, Z.; EMANUEL, E. J. Predicting the future — big data, machine learning, and clinical medicine. New England Journal of Medicine, vol. 375, no. 13, 2016, pp. 1216–1219.Link
- EUROPEAN PARLIAMENT AND COUNCIL. Regulation (EU) 2024/1689 of the European Parliament and of the Council of 13 June 2024 laying down harmonised rules on artificial intelligence (Artificial Intelligence Act). Official Journal of the European Union, L series, 2024. Available at: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=OJ:L_202401689Link
- U.S. FOOD AND DRUG ADMINISTRATION (FDA). Artificial Intelligence and Machine Learning (AI/ML)-Based Software as a Medical Device (SaMD) Action Plan. Washington, D.C.: FDA, 2021. Available at: https://www.fda.gov/medical-devices/software-medical-device-samd/artificial-intelligence-and-machine-learning-aiml-based-software-medical-device-samdLink
- WORLD HEALTH ORGANIZATION (WHO). Ethics and Governance of Artificial Intelligence for Health: WHO Guidance. Geneva: WHO, 2021. Available at: https://www.who.int/publications/i/item/9789240029200Link
- TOPOL, E. J. Deep Medicine: How Artificial Intelligence Can Make Healthcare Human Again. New York: Basic Books, 2019. ISBN 978-1541644649.